Much to the chagrin of the astrology experts, Shakespeare had a thing to say about it, “It is not in our stars to hold our destiny but in ourselves.” So what is in ourselves that we need to look at?

Interestingly, plenty of stuff!

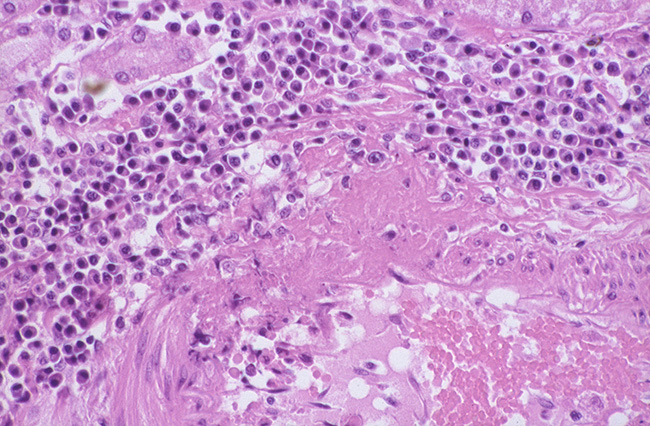
In the 1990s there were articles about the importance of the presence of lymphocytes infiltrating the cancerous tissue. Physicians looked at these findings and compared outcomes with and without the presence of lymphocytes. They came away with the unassailable thought that the presence of the lymphocytes had some positive impact on survival. In early stage II/III colorectal cancer for instance they were able to determine that the presence of tumor infiltrating lymphocytes (TILs) in the tumor tissues were associated with longer term survival. Curious indeed, but at that time the tools were not there to study them further.
In Melanoma for instance a similar viewpoint held that TILs helped improve a person’s chances in overcoming the disease. In Melanoma, however, the immunity issue became a singular focus for a long time. Treatments included Interferon therapy, Interleukin-2 (as well in Renal Cel cancer) therapy and Vaccination against the epitope on the melanoma cells. These treatments were quite debilitating in nature, giving symptoms of a aggressive “Flu-like syndrome” each time the patient received the IFN or IL-2. One had to get the Interferon shot daily for 30 days, then three times a week for a year. It wreaked havoc on the patient, but there were responses. People not supposed to live, survived.


Breast Cancer data also seemed to suggest the presence of TILs in the surrounding tissue of the cancer. Little evidentiary information has been gathered or experimented in this malignancy, however, since there are much better methods of treatment available for this malady.
Modern Medicine dating back five or so years has resurrected the whole TIL concept once again and it seems successfully given another kick in the pants.

Knowing that the composition of the lymphocytes is T cells, B cells, NK (Natural Killer) cells, Helper Cells, Dendritic Cells that sample the antigen and macrophages, medicine has figured out how to manipulate the immune system in those patients that have an army of these TILs lurking around the tumor tissue. Since these cells are present, it is obvious that they have sampled the antigen on the cancer cells and having done so, if one were to enhance their effect, one could gain another foothold against this scourge called “The emperor of Maladies.”
Further knowledge development from studying this cellular machinery revealed that the cancer cells have accommodated this immune onslaught quite successfully by using the cell’s own defense mechanism of cloaking their anticancer activity with a protein. This protein, the scientists realized, was preventing the immune function from destroying the tumor. From the alternate point of why, one might ask, why does the body not want to protect itself? The answer was clear, allowing a rampant immune response without any checkpoints would lead the body to “destroy” itself when attacked by a simple infection, akin to a pleasant breeze turning into a hurricane. So checks and balances needed to be present to prevent such hyperbolic activity.

Well now having delineated the mechanisms of action the Immune brigade can be carefully turned against the cancer itself. First the presence of the TILs is an important precursor to the present thinking. The determination of the protein called PD-1 (receptor on the lymphocyte that limits its anticancer function) and PD-L1 (the receptor present on the cancer cells itself). Inhibiting the function of these receptors has resulted in a plethora of drugs armed and aimed at these two proteins (the guardians against hyperbolic responses). Once the checkpoint has been blocked the immune cells can go on to demolish the enemy (cancer). It goes without saying; the more the TILs the better the body is equipped to be helped or conversely if the disease is advanced with a large tumor burden and low to absent TILs, the lower the chances of response.

We tread slowly towards a better future and I end with Shakespeare again, “ Wisely and slow. They stumble that run fast.”
References:
Adam, S et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J Clin Oncol. 2014 Sep 20;32(27):2959-66.
https://www.researchgate.net/profile/Claudio_Clemente/publication/14591062_Clemente_CG_Mihm_Jr_MC_Bufalino_R_Zurrida_S_Collini_P_Cascinelli_NPrognostic_value_of_tumor_infiltrating_lymphocytes_in_the_vertical_growth_phase_of_primary_cutaneous_melanoma._Cancer_77_1303-1310/links/541c00f00cf203f155b34fb0.pdf
http://www.cancernetwork.com/oncology-journal/high-dose-interleukin-2-it-still-indicated-melanoma-and-rcc-era-targeted-therapies
http://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-015-0431-3
http://jnci.oxfordjournals.org/content/108/11/djw144.short













No comments:
Post a Comment