The beast within grows. Its white fangs and long curled
talons seem like a caricature in a sci-fi movie, than real life. But there it
is, the Gryphon, baring its teeth encrusted beak and its hawkish eyes under the brown and
white ruffled feathers that spell dominance. The creature is restless, as its
deep-dark eyes dart from side to side.
The SGR seems oddly to fit the image of this beast. Born of
a thought for containment, as a dovish sort of benevolent bird, flitting about
from tree to tree, it has eaten off the forbidden fruit of procrastination and
turned into this giant beast of hawk-like demeanor with a reptilian
cold-blooded calculating mind-set.
What is SGR (Sustained Growth Rate) formula after all?
The Medicare Sustainable Growth Rate (SGR) is currently used
by the CMS Centers for Medicare and Medicaid Services in the United States to
control spending by Medicare on physician services. The SGR was enacted by the Balanced Budget Act of 1997 to amend Section 1848(f) of the Social Security Act and replaced the Medicare Volume Performance Standard (MVPS). CMS previously
used MVPS in an attempt to control costs. Generally, this is a method to ensure
that the yearly increase in the expense per Medicare beneficiary does not
exceed the growth in GDP.

“Every year, the CMS sends a report to the Medicare Payment Advisory Commission, which advises the US Congress on the previous year's total expenditures and the target expenditures. The
report also includes a conversion factor that will change the payments for
physician services for the next year in order to match the target SGR. If the
expenditures for the previous year exceeded the target expenditures, then the
conversion factor will decrease payments for the next year. If the expenditures
were less than expected, the conversion factor would increase the payments to
physicians for the next year.”
The four factors involved in these calculations include:
1. The estimated percentage change in fees for physicians’
services.
2. The estimated percentage
change in the average number of Medicare fee-for-service beneficiaries.
3. The estimated 10-year average annual
percentage change in real GDP per capita.
4. The estimated percentage change
in expenditures due to changes in law or regulations.
As one can guess, given this oddly figured attempt to
control healthcare costs, the physicians are being used as the “sacrificial
lambs.” While on one side there is a “push” to invest in conforming to
regulatory requirements and added jungle of complexity, which any kindergarten
student will tell you, adds to the costs of care, the other side is hell-bent
on “you can’t raise prices!” The only thing
close to reality would be telling McDonald Restaurants to have seating for
hundred customers in each restaurant and hire 20 extra employees to service the
stations and oh but you (McDonald) cannot raise the prices of hamburgers. Hmm…

And here is a real world personal example: When I first
started practicing medicine, I had one employee. She was the front-office and
did everything else except practice medicine. Then as time expanded and as
needs grew, my office expanded the workforce to two and then three and before,
I had a chance to realize it, I had 10 workers staffing a one-physician
facility. There was a billing person, a coder, an insurance pre-qualifier, two
nurses, a chart filer, a front office receptionist, an office manager and two
laboratory technicians. Not to mention other contractors for computer services,
OSHA regulatory compliance, COLA and CLIA regulatory compliances. So all in
all, keeping this large workforce to continue providing healthcare services
required a larger revenue stream. The SGR creators on the other hand remained
distant and oblivious to the external forces enacted by the congressional
experts that were constantly shaping and adding the streams of burden on a
physician’s abilities. The simple act of comprehension seemed oddly absent in
the mix of these “experts.” The one hand continues to harvest “nothing” while
the other hand continues to “seed” something; simultaneity of complex idiocy.
While the Congress and the Executive branches have been
reviewing the burgeoning “big” data based on a falsified premise, and believing
in it’s virtues they have nevertheless continued to “kick the can down the
road.” Already in arrears for -27.4% over the past decade, there is very little
“stomach” to stomach the potential “backlash” from the physician and patient
advocacy groups. Both will lose a large number of care-givers and care-needy numbers.
And if the new movement of rising numbers of “hospitalists” (physicians
employed by the hospitals to render inpatient care) is a comfort to society,
the SGR follows the physician wherever he goes and that brings the hospital
revenues under scrutiny and potential pressure. The AHA lobbyist are already at
it, spinning their intellectual wheels to find the cure for this contagion. And the beat goes on...
The vitriol continues about the “rich doctors” and their
lifestyles of big houses and
expensive cars, as the clarion call to rally the masses in support of the
impending cuts continues. Yet even this weary class-envy seems not to bring in
the desired angst from the populace, for they fear a loss of “something” for
themselves. The “warfare” against physicians continues while the public “servants” fly around
under Rolls Royce powered jets from halls of congress to their districts and
are wined and dined by corporate magnates to enforce the cuts so that larger
portions of the insurance premiums become the incremental added share-value.
Ah! But I digress!
So here we are delaying the inevitability based on the
faulty premise to begin with. Yet this delay diverts the consequences from now
to the future where the pain will be greater and survivability not insured.
This persistent delay will rear its ugly head as a rampant inflation of a
dislocated reality where healthcare will suffer at the alter of fewer
physicians and many “compliance czars” that mete out the marginalized healthcare.
Ron Shinkman of Fierce Health Finance states,
“As a result, doctors are facing a 27.5 percent cut in
payments for the care they provide--the accumulation of a decade of cost
deficits that have never been addressed. It's a deeply ludicrous cut and will
never happen, but it exists solely because of past inaction.
Meanwhile, as the Affordable Care Act takes greater hold
in 2014 and the years after, there is likely going to be more pressure to keep
the healthcare cost curve down. If Massachusetts, the ACA's original home, is
any guide, inflation is going to move up from its current historical lows
pretty quickly.
A variety of health policy experts have noted the SGR
tug-of-war has kept the physician community from focusing on properly
implementing reform.”
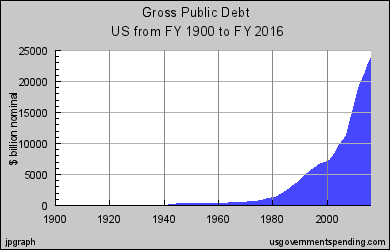
US Federal Debt ~ Projected
United States Public Debt
Let us briefly cast our view on the world of finance, it is
akin to the “doc-fixes” that have been implemented over the past ten years. There
is no appetite for risk. No appetite for new beginnings, just the same old “kick
the can,”
experience. The Non-risk takers have ensconced themselves and now lord over the
risk-takers. “Nothing can be done that rattles any person,” is the rallying cry. The political
correctness sting is on. And what this begets is a future that follows. Greece is a perfect example of this glorified
pervasive European dysfunction that seems so desirous in the United States.
Greece is only a “Nein!” away (no more free Euros from the working class) from
devolving into anarchy and chaos, followed closely by Spain and then Italy. A
US debt to the tune of $16, 337,000,000,000.00 where almost $950,000,000,000
are paid out as interest annually is 104% of the GDP (Gross Domestic Product).
And should you desire to know, Greece is at 178.4%. Spain is at 90.4% and
although that might be comforting to some, it is also wiser to know that Brazil
and Mexico both defaulted with debts to GDP ratios of 50%.

The Greek Debt to GDP
Greece GDP
Getting back to the Mediscare called SGR formula, the
essence of this ensuing debacle lies squarely on the inefficiencies of a
bureaucracy that allows for exploitation by the bad elements in society, A
payment formula based more on the “lobbyists-determinant” rather than the
actual cost and a “ivory-tower” controlled by the non-risk-takers who manage
the levers of control, compare and contrast.
Are there inefficiencies in healthcare? Yes!
Are there better methods of delivery of healthcare? Yes!
Are there efficiencies that can be exploited to benefit the
system? Yes!
The one-word answers exist in the Risk-Taker realm but not
in the exploiting bookish world of “experts.” Just like an economist (Nobel
Laureate or not) who has never balanced a checkbook will never know the levers
that govern the real world. The consequence of an action is never contemplated
by these rarified few. An expert high up in this “high-up” world of “do this…” has no concept of how medicine is
really practiced or for that matter how the world really works or the costs
that are incurred and what will be the rip-tide consequences of that "do this..." They just sit and profess…
Ignoring these precarious risks, with vacant eyes, of the
beast that lurks is forbearance of what is to come.
Meanwhile the fangs and talons get bigger and bigger and the tail whips and whips hungrier and hungrier...
References:
SGR Formula
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SustainableGRatesConFact/index.html?redirect=/SustainableGRatesConFact/
Medicare Volume Performance Standard (MVPS)
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SustainableGRatesConFact/downloads/sgr2010f.pdf
Medicare beneficiary expense and the GDP
http://blogs.wsj.com/health/2008/07/10/why-medicare-pay-cuts-for-doctors-will-be-back/
SGR and the “Cliff” ~ Ron Shinkman
SGR faces its
own fiscal cliff - FierceHealthFinance - Health Finance, Healthcare Finance
http://www.fiercehealthfinance.com/story/sgr-faces-its-own-fiscal-cliff/2012-12-11#ixzz2GSwwKnpC
The Sovereign Debt Crisis: A modern Greek tragedy (Federal
Reserve Bank of Saint Louis)
http://www.stlouisfed.org/publications/cb/articles/?id=2264